› Forums › General Melanoma Community › Questions and Answers from Jim In Denver Co..Melanoma..Jim Breitfeller
- This topic has 8 replies, 3 voices, and was last updated 15 years, 9 months ago by
jim Breitfeller.
- Post
-
- October 22, 2010 at 2:39 pm
Jim,
First of all thank you for replying to my post. I usually don’t get many replies. When I talk to my wife about this, within the first five minutes she is telling me “I am loosing her.” It has taken me close to three years to get to where my knowledge on melanoma and the immune system is today. I don’t mean to talk over patient heads. It is just the scientist in me. I worked at Eastman Kodak’s Research laboratories for 25 years.Now to answer you first question:
Jim,
First of all thank you for replying to my post. I usually don’t get many replies. When I talk to my wife about this, within the first five minutes she is telling me “I am loosing her.” It has taken me close to three years to get to where my knowledge on melanoma and the immune system is today. I don’t mean to talk over patient heads. It is just the scientist in me. I worked at Eastman Kodak’s Research laboratories for 25 years.Now to answer you first question:
You have said that the most effective durable treatment for advanced melanoma would consist of Ipilimumab combined with IL2 – is that correct?
Based on my research today, IL-2 and Anti-CTLA-4 (Ipilimumab) are most durable as we speak. A new phase I therapy is showing great promise with less side effects. That is anti-PD-1 Therapy. These therapies don’t need a specific HLA type to get into the trials.
There is also a very, very ,very new therapy that is still in translational stage. Translational research is a way of thinking about and conducting scientific research to make the results of research applicable to the population under study and is practised in the natural and biological, behavioural, and social sciences. It is usally conduted with animals like rats, mice, monkies.
Anyway this therapy combines the Anti-CTLA-4 and Anti-PD-1. It has shown syenergnic results.
If you have c-Kit or BRAF mutations, then targeted therapy may used but may not be durable.
If you are HLA-02 Positive, You have the option of ACT therapy with Dr. Rosenberg or Dr. Patrick Hwu at NCI or MD Anderson. They have gotten 72 % response rate with I think about 36 % complete response is I am not mistaken.
Second Question:
There are no studies currently availble that combine Ipi and IL2, is that correct?
Define combine? There was a clinical study done by Dr. Rosenberg and colleages.
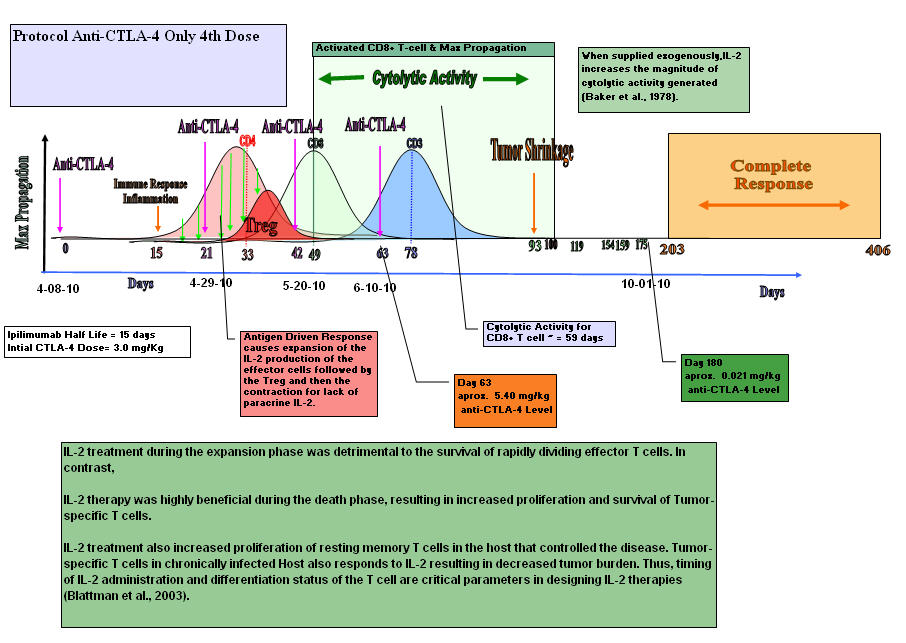
As you can see in the graph above, IL-2 was added prior to the maximum propagation of the CD4+ T helper cells. IL-2 is known as a growth factor. So what I believe happened in this trial, they grew the Tregs.
IL-2 treatment during the expansion phase was detrimental to the survival of rapidly dividing effector T cells. In contrast, IL-2 therapy was highly beneficial during the death phase, resulting in increased proliferation and survival of Tumor-specific T cells. IL-2 treatment also increased proliferation of resting memory T cells in the host that controlled the disease. A tumor-specific T cell in chronically infected Host also responds to IL-2 resulting in decreased tumor burden. Thus, timing of IL-2 administration and differentiation status of the T cell are critical parameters in designing IL-2 therapies (Blattman et al., 2003).
So what I am trying to say is you do the Ipilimumab therapy first. Wash out for about 50 days, and then start IL-2 Therapy.
Take away: It is a systemic combination with dosing and timing involved. Systemic Combinatorial Therapy.
Question 3:
If someone were to choose to do a combination treatment on their own (i.e. get IL2 following a course of Ipi through one of the clinical trials), would there be an advantage
to starting IL2 as soon as possible after stopping Ipi? Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?Base on papers from ITOH etal and others, 49 days after activation is at the maximum growth phase for the CD8- T-cells that mature into Cytotic T Lymphocytes.
<strong>Results: Graph setup</strong>
Kinetic Study of rIL-2-induced Expansion. In all 12 metastatic melanomas tested, a substantial proportion of TIL was present in tumor cell suspensions.
The ratio of lymphocytes to tumor cells ranged from 0.03 to 1.25 with an average ratio of 0.40 t 0.37. By fluorescence analysis,
TIL consisted of 78 days 11% CD3
T cells, 33 days 10% CD4+
<strong>T cells, 49 days 17% CD8+</strong>
Their CD4/CD8 ratio was 0.67.
(ITOH et al., 1988)It was also reported that there is a time factor involved.
Our results show that T4 + human T cells differ substantially from T8 + cells with respect to their IL-2 responsiveness. T4 + cells cease to proliferate well before T8 + cells during a primary response. (GULLBERG AND SMITH et al.,1986)<strong>Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?</strong>
Yes, Ipilimumab has a half life of 15 days. So say you get one dose at 3.0 mg/Kg.
Days– concentration
0– 3
15– 1.5
30– 0.75
45– 0.375
60– 0.1875
75– 0.09375
90– 0.04687
105– 0.02343
120– 0.01171
135– 0.00587
150– 0.00292
165– 0.00146
180– 0.00073It gets more complicated when you get multiple doses. Four dose regiment.
Days– concentration
0– 3
15– 1.5
30– 3.7
45– 4.85
60– 5.425
75– 2.7125
90– 1.35625
105– 0.68
120– 0.34
135– 0.17
150– 0.08
165– 0.04
180– 0.021I am not sure where the limited threshold is but, at day 49 you have close to the maximum concentration of Ipilimumab in your body.
Since I used Tremelimumab with Half Life = 21 days and did 15mg/Kg
I had at day 50 approximately 2.17 mg/Kg anti-CTLA-4 level in my body
<strong>If I had to venture an educational guess, I would say after a four dose regime, you have 75 days to do the HD IL-2.</strong>
To back this theory up, we will use a chart from Dr. Wolchok experience the Ipilimumab.
It is a chart with the Absolute Lymphocyte count. (ALC). It is the CD4+ T-cells and CD8+ T cells combined.

As you can see from the graph, the maximum ALC was about week 7.
Week seven correlates to 49 days. That is when CD8+ T cells are at their maximum growth.Question 4:
Last, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi?
This my take on the situation. You need the <strong>tumor-specific antigen</strong> to presented to the T-cells as signal 1. That could be a vaccine, radiation therapy or chemo to shed the antigen.
<strong>Secondly you need the costimulation of the CD28/B7 interface</strong>. By using Ipilimumab that blocks the CTLA-4 receptor from binding to the B7 molecule and shutting down the response.
Anti-CTLA-4 (ipilimumab) also blocks the CTLA-4 receptor on the Treg cells subduing their surpress function.Third you need a “Danger Signal” to get the cell to migrate to the tumor site. This may be done with inflammatory Cytokines like IL2, IL17, IL-1,IL-12,IFN gamma that act directly on the T-cells. This signal was found to optimally activate the Th1 differentiation and lead to the clonal expansion of the T-cells.
It has come to light recently that Ipilimumab helps also in the differentiation by tilting the balance towards Th17 cells. These cells secrete IL-17 which recruite the neutrophils. This all takes place at the tumor’s microenviroment. The neutrophils secrete chemokines that are chemoattractants.These chemokines, MIP-1alpha, MIP-1beta, and MCP-1 are recently reported to serve as chemoattractants for Th1 cells. MIP-1alpha and MCP-1 are also reported to enhance antigen-specific (CTL) Cytotoxic T Lymphocyte induction. Studies revealed that MIP-1alpha /beta released from neutrophils are involved in recruitment of macrophages, T cells, monocytes, dendritic cells (DC), neutrophils and NK cells.
MIP-1 attracts predominantly CD8+ T cells while MIP-1 attracts CD4+ cells, although there is some overlap between subsets in response to both chemokines.
The other Chemokine MCP-1, binds to CCR2 to accumulate monocytes/macrophages, DC, T cells, and NK cells, thereby playing an important role in innate and adaptive immunity. CCR2 is Chemokine receptor that is key determinant of leucocyte trafficking.IL-2 strongly upregulates expression of CCR2. With the MCP-1/CCR2 interface, the cells can traffic towards the tumor’s microenvironment. The trafficking of the cells and inflammatory cytokines present the perfect storm in the tumor’s microenvironment to induce the right immune response to eradicate the cancer, Melanoma.
So to answer your question, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi? yes if you know and take a systemic approach. You need to activate the t-cells before introducing IL-2. IL-2 can be the activator for small patient population.As for Ipilimumab going it alone, like IL-2 can be the activator for small patient population. But when you do a systematic combinatorial therapy, there can be a synergetic result, complete response.
I hope I answered you questions, and please don’t hesitate to ask them. I do all this time by requesting reseach papers from around the world. Each question is a learning tool. There are no stupid questions. Knowledge is power to make an educated decision. Your Life may depend on it. There are many paths to take. Just follow the yellow brick road to complete response.
“It is not the strongest of the species that survives, nor the most intelligent, but the one most responsive to change.”
~Charles Darwin~
Take Care,
Jimmy B
- Replies
-
-
- October 22, 2010 at 3:01 pm
Jim,
Sorry about the formatting. I posted it on Melanoma Missionary, which the formatting is fine.
Please let me Know if you have any other questions. Don't be afraid to ask. There are no wrong questions.
Have a great day
Jimmy B
-
- October 22, 2010 at 4:23 pm
Hi Jimmy,
Thank you so much for you prompt, detailed, an thoughtful replies to my questions. I now need to read and reread your answers, and may have followup questions later. I am aware of your scientific background, which has helped enabled you to comprehend the sometimes mind-numbing science behind melanoma research. I greatly respect your knowledge and dedication to helping the rest of us decipher current research data, and assist in helping us make informed decisions.
I think the reason that you may not receive more questions from the board is that there is a sense that you are operating on a higher plane of knowledge and understanding that most of the rest of us, and that we may not understand enough to ask intelligent questions. You are very generous to offer to help myself and others, and I have been impressed from my first days on the board with your work on our behalf. Your wife should know that you are helping make a significant difference to others with melanoma, though you may not have not recieved sufficient positive feedback about that fact.
The reason I asked these particular questions at this time is because I am working to develop my own treatment plan, and considering alternative treatment paths for myself, which depend on what my next set of scans show next week. You may recall I am enrolled in the Ipi/Temodar trial at MDA, and am at the end of the "Induction Phase".
Many Thanks,
Jim
-
- October 22, 2010 at 4:23 pm
Hi Jimmy,
Thank you so much for you prompt, detailed, an thoughtful replies to my questions. I now need to read and reread your answers, and may have followup questions later. I am aware of your scientific background, which has helped enabled you to comprehend the sometimes mind-numbing science behind melanoma research. I greatly respect your knowledge and dedication to helping the rest of us decipher current research data, and assist in helping us make informed decisions.
I think the reason that you may not receive more questions from the board is that there is a sense that you are operating on a higher plane of knowledge and understanding that most of the rest of us, and that we may not understand enough to ask intelligent questions. You are very generous to offer to help myself and others, and I have been impressed from my first days on the board with your work on our behalf. Your wife should know that you are helping make a significant difference to others with melanoma, though you may not have not recieved sufficient positive feedback about that fact.
The reason I asked these particular questions at this time is because I am working to develop my own treatment plan, and considering alternative treatment paths for myself, which depend on what my next set of scans show next week. You may recall I am enrolled in the Ipi/Temodar trial at MDA, and am at the end of the "Induction Phase".
Many Thanks,
Jim
-
- October 22, 2010 at 3:01 pm
Jim,
Sorry about the formatting. I posted it on Melanoma Missionary, which the formatting is fine.
Please let me Know if you have any other questions. Don't be afraid to ask. There are no wrong questions.
Have a great day
Jimmy B
-
- October 23, 2010 at 12:13 am
Very impressive post. I think you did a great job of posting a detailed explaination that was decipherable by us lamens. There are so many possibilites that are so exciting, I just wish they could come to fruition quicker and with less red tape. we should make this post a sticky and keep it at the top.
– pat on li
-
- October 23, 2010 at 12:13 am
Very impressive post. I think you did a great job of posting a detailed explaination that was decipherable by us lamens. There are so many possibilites that are so exciting, I just wish they could come to fruition quicker and with less red tape. we should make this post a sticky and keep it at the top.
– pat on li
-
- October 23, 2010 at 12:36 am
Pat and Jim thanks for the positive feed back. I am going to share with you a post from my Melanoma Journey.
6/23/2006
I had a quite a busy Thursday night and Friday. I don’t know where to begin but I will try. Thursday night, I was frustrated from trying to reach doctors all day. I got a call from my sister, Jody, who gave me the name of a Dr. Weber in California who treated an old friend of hers for melanoma. So I called him, and talked to him about the trial I signed on for. He felt the trial was inappropriate as a first line of defense. This was right in line with what the doctors in Pittsburgh said. They all felt is was more of a last resort treatment. Sooooo, of course I went into a ridiculous panic. Frantically, I began trying to reach my oncologist here in Rochester to opt out of the trial. Fearful that I signed my life away, I was prepared to run and hide from him if necessary. (When my wife came home she pointed out that there was a disclaimer enabling me to stop the trial at any time.) Whew!!!! The oncologist didn’t return my call—and the office was now closed. (Who closes at 4:30? That’s better than banker’s hours!) My next meeting with him would be 5 days away, and I needed to rectify the situation or I would not be getting any sleep. Then it occurred to me—where do you go after closing? Home, of course. So I picked up the white pages and began scanning through the names/numbers. Sure enough, his name and home address were listed. I dialed the number and his wife answered. Ooooh, was SHE peeved! But she passed the phone to my doctor. When he got done yelling at me, (he said he was not on call, and I should be calling the phone service…) he filled me in on the info he should have called me about earlier in the day. Apparently, he had had a conversation with Pittsburgh docs regarding the best paths to take. But he didn’t tell me everything. He said to call back at the office in the morning…
Not satisfied, first thing Friday, I couldn’t wait, so I called the Pittsburgh Doctor’s pager at 6am. (He had slipped that he awakens at 4:30 every day, so I figured I’d reach him.) He was kind enough to call and fill me in at that ungodly hour.
On Friday afternoon, I met the boy’s (the Kodak trio—three retired gentlemen who provided me with transportation to/from the hospital for my treatments, recently) at Silk’s for lunch. You probably know the place. Also referred to as O'Laughlin's, it is located on the river at the end of St. Paul Blvd.I was waiting for a phone call from the doctor, so I took my wife’s cell phone with me. We were enjoying lunch on the patio, and one of the guy’s said “Hey, the bikers should be arriving anytime now.” Just then, the cell rang. It was the doctor calling with the information I’ve been waiting for about the clinical trials I have to choose from. Suddenly a roar of noise rolled into the parking lot. I can only imagine what the doctor was thinking about my whereabouts. . . but somehow she managed to communicate the information to me.
I have a choice of 28 trials to choose from. 10 are particularly appropriate for me. And of the 10, 4 would be considered a good first line of defense. I don’t have a lot of detail, but my next appointment is in Pittsburgh on Wednesday. That’s when each of the choices will be explained in detail. Depending on which therapy we go with, I may actually be able to arrange to have the treatments here and go back to Pittsburgh only once a week or once every two to three weeks. This is good news, since even the Family Houses in the area cost $25 to $30 per night… this could add up fast!
At that time i was a rookie in how the process works. I come a long way baby!!!!. It was so overwhelming when I first got ill. So I know first hand on what all the MPIP patients are going through. If you make the wrong choice it could shut you out of a trial that could save your life. I call it Bio-Chess and we are the Pawns that are expendable according to science.
So ask away. I don't know every thing, but As Dr. Casey Culberson Said:
"The BEST melanoma patient is an ACTIVE PARTICIPANT in his or her treatment
(not a PASSIVE RECIPIENT)"Take care
Jimmy B
-
- October 23, 2010 at 12:36 am
Pat and Jim thanks for the positive feed back. I am going to share with you a post from my Melanoma Journey.
6/23/2006
I had a quite a busy Thursday night and Friday. I don’t know where to begin but I will try. Thursday night, I was frustrated from trying to reach doctors all day. I got a call from my sister, Jody, who gave me the name of a Dr. Weber in California who treated an old friend of hers for melanoma. So I called him, and talked to him about the trial I signed on for. He felt the trial was inappropriate as a first line of defense. This was right in line with what the doctors in Pittsburgh said. They all felt is was more of a last resort treatment. Sooooo, of course I went into a ridiculous panic. Frantically, I began trying to reach my oncologist here in Rochester to opt out of the trial. Fearful that I signed my life away, I was prepared to run and hide from him if necessary. (When my wife came home she pointed out that there was a disclaimer enabling me to stop the trial at any time.) Whew!!!! The oncologist didn’t return my call—and the office was now closed. (Who closes at 4:30? That’s better than banker’s hours!) My next meeting with him would be 5 days away, and I needed to rectify the situation or I would not be getting any sleep. Then it occurred to me—where do you go after closing? Home, of course. So I picked up the white pages and began scanning through the names/numbers. Sure enough, his name and home address were listed. I dialed the number and his wife answered. Ooooh, was SHE peeved! But she passed the phone to my doctor. When he got done yelling at me, (he said he was not on call, and I should be calling the phone service…) he filled me in on the info he should have called me about earlier in the day. Apparently, he had had a conversation with Pittsburgh docs regarding the best paths to take. But he didn’t tell me everything. He said to call back at the office in the morning…
Not satisfied, first thing Friday, I couldn’t wait, so I called the Pittsburgh Doctor’s pager at 6am. (He had slipped that he awakens at 4:30 every day, so I figured I’d reach him.) He was kind enough to call and fill me in at that ungodly hour.
On Friday afternoon, I met the boy’s (the Kodak trio—three retired gentlemen who provided me with transportation to/from the hospital for my treatments, recently) at Silk’s for lunch. You probably know the place. Also referred to as O'Laughlin's, it is located on the river at the end of St. Paul Blvd.I was waiting for a phone call from the doctor, so I took my wife’s cell phone with me. We were enjoying lunch on the patio, and one of the guy’s said “Hey, the bikers should be arriving anytime now.” Just then, the cell rang. It was the doctor calling with the information I’ve been waiting for about the clinical trials I have to choose from. Suddenly a roar of noise rolled into the parking lot. I can only imagine what the doctor was thinking about my whereabouts. . . but somehow she managed to communicate the information to me.
I have a choice of 28 trials to choose from. 10 are particularly appropriate for me. And of the 10, 4 would be considered a good first line of defense. I don’t have a lot of detail, but my next appointment is in Pittsburgh on Wednesday. That’s when each of the choices will be explained in detail. Depending on which therapy we go with, I may actually be able to arrange to have the treatments here and go back to Pittsburgh only once a week or once every two to three weeks. This is good news, since even the Family Houses in the area cost $25 to $30 per night… this could add up fast!
At that time i was a rookie in how the process works. I come a long way baby!!!!. It was so overwhelming when I first got ill. So I know first hand on what all the MPIP patients are going through. If you make the wrong choice it could shut you out of a trial that could save your life. I call it Bio-Chess and we are the Pawns that are expendable according to science.
So ask away. I don't know every thing, but As Dr. Casey Culberson Said:
"The BEST melanoma patient is an ACTIVE PARTICIPANT in his or her treatment
(not a PASSIVE RECIPIENT)"Take care
Jimmy B
-
Tagged: cutaneous melanoma
- You must be logged in to reply to this topic.