› Forums › General Melanoma Community › What we can learn from individual patients is often overlookedin oncology
- This topic has 2 replies, 1 voice, and was last updated 15 years, 9 months ago by
Jim in Denver.
- Post
-
- October 21, 2010 at 4:48 pm
 "What we can learn from individual patients is often overlookedin oncology he said, adding that many of these remarkablecases have led to the development of new treatment strategiesfor melanoma such as vaccinations against specific antigensand bone marrow transplantation. "From clinical observation,we can learn a lot from these remarkable cases," he said"What we can learn from individual patients is often overlookedin oncology he said, adding that many of these remarkablecases have led to the development of new treatment strategiesfor melanoma such as vaccinations against specific antigensand bone marrow transplantation. "From clinical observation,we can learn a lot from these remarkable cases," he said
"What we can learn from individual patients is often overlookedin oncology he said, adding that many of these remarkablecases have led to the development of new treatment strategiesfor melanoma such as vaccinations against specific antigensand bone marrow transplantation. "From clinical observation,we can learn a lot from these remarkable cases," he said"What we can learn from individual patients is often overlookedin oncology he said, adding that many of these remarkablecases have led to the development of new treatment strategiesfor melanoma such as vaccinations against specific antigensand bone marrow transplantation. "From clinical observation,we can learn a lot from these remarkable cases," he saidAlan Houghton, M.D., chiefof immunology at Memorial Sloan-Kettering Cancer Center, NewYork
AS I continue my research I am uncovering amazing things about out immune system. If you don't get an immune response, you might be missing the "Danger Signal"
Three major events must occur to induce CD8+ T cell–mediated, tumor-protective immunity against melanoma
First , the T-cell receptor must be triggered by a (or multiple) self antigen–derived peptide MHC class I complex. Therefore, this event depends entirely on appropriate antigen presentation, which is most efficiently provided by mature dendritic cells. Peripherally tolerant or “ignorant” self-reactive T-cell clones, once properly activated, may serve as tumor-specific effector T cells.
Second, simultaneously with T-cell receptor triggering, a distinct second costimulatory signal must be delivered, mediated by IL-2, B7-1, or B7-2, which engage IL-2 receptors and CD28 on the surface of the T cell, respectively (17). A source of these cofactors for effective CD8+ T-cell stimulation can be provided by CD4+ T cells that release critical amounts of IL-2, or by mature dendritic cells that display an increased level of B7-1/B7-2 costimulatory molecules on their cell surfaces.
Third, inflammatory cytokines, including IL-1, IL-6, IL-12, and IFN-γ provide a third signal that acts directly on T cells, referred to as the “danger signal”. This signal was found to optimally activate TH1 differentiation and lead to clonal expansion of T cells.1
The inflammatory cytokines act to promote T cell responses. They include IL-1, IL-6, IL-12, TNF-α, and IFN-g produced by macrophages and/or dendritic cells. Th17 cells also plays a part by secreting IL-17 and others. The most notable role of IL-17 is it involvement in inducing and mediating proinflammatory responses. Neutrophils are the earliest cells to arrive at the inflammatory site.
While TGF-β is a critical differentiation factor for Treg cells, IL6 completely inhibits the generation of Treg cells induced by TGF-β. Instead, IL6 and TGF-β together induce the differentiation of pathogenic Th17 cells. With IL-6 missing in the microenvironment, Treg Cells flourish.
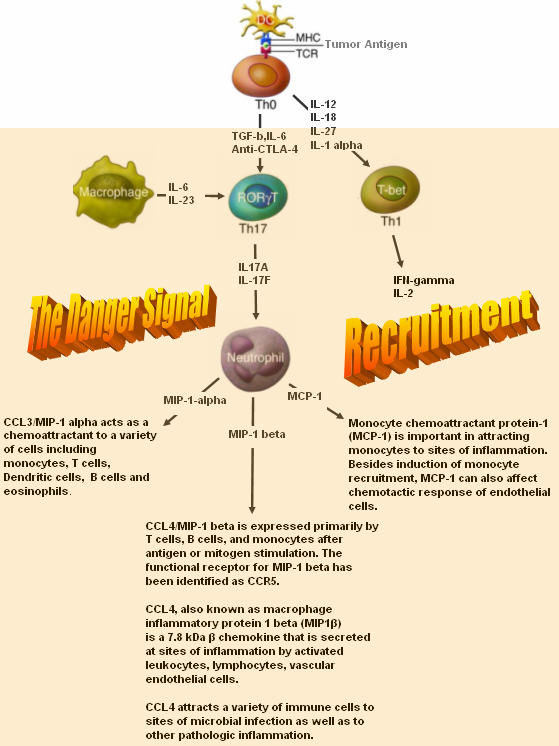 Anti-CTLA-4 blockage tilts the balance of the differentation of the T helper cells toward the Th17 phenotype. Once at the Tumor's microenviroment, it secretes IL-17, an inflammatory cytokine. This cytokine attracts the neutrophils cells to the tumor site. It then secretes chemoattractants, MIP-1 alpha, MIP-1 beta and MCP-1.
Anti-CTLA-4 blockage tilts the balance of the differentation of the T helper cells toward the Th17 phenotype. Once at the Tumor's microenviroment, it secretes IL-17, an inflammatory cytokine. This cytokine attracts the neutrophils cells to the tumor site. It then secretes chemoattractants, MIP-1 alpha, MIP-1 beta and MCP-1.These chemokines, MIP-1alpha, MIP-1beta, and MCP-1 are recently reported to serve as chemoattractants for Th1 cells. MIP-1alpha and MCP-1 are also reported to enhance antigen-specific (CTL) Cytotoxic T Lymphocyte induction. Studies revealed that MIP-1alpha /beta released from neutrophils are involved in recruitment of macrophages, T cells, monocytes, dendritic cells (DC), neutrophils and NK cells.
MIP-1 attracts predominantly CD8+ T cells while MIP-1 attracts CD4+ cells, although there is some overlap between subsets in response to both chemokines.The other Chemokine MCP-1, binds to CCR2 to accumulate monocytes/macrophages, DC, T cells, and NK cells, thereby playing an important role in innate and adaptive immunity. CCR2 is Chemokine receptor that is key determinant of leucocyte trafficking.
IL-2 strongly upregulates expression of CCR2. With the MCP-1/CCR2 interface, the cells can traffic towards the tumor’s microenvironment. The trafficking of the cells and inflammatory cytokines present the perfect storm in the tumor’s microenvironment to induce the right immune response to eradicate the cancer, Melanoma.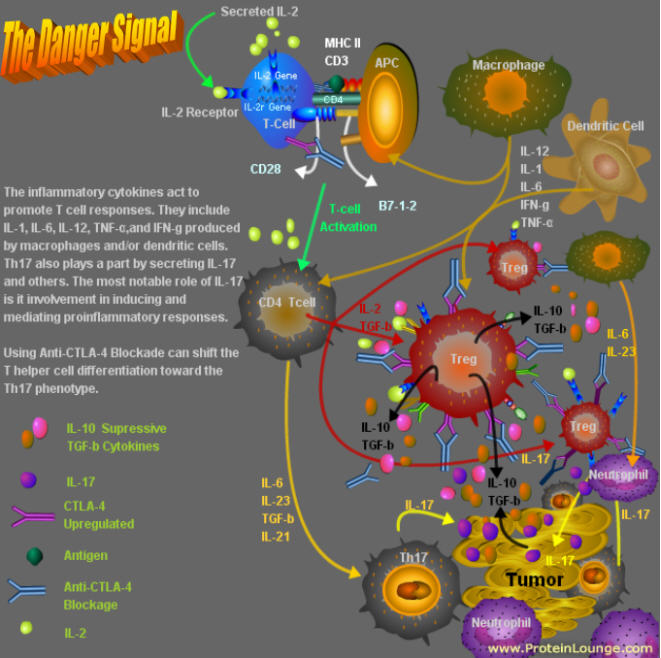
I thought you might want to know,
Jimmy B
- Replies
-
-
- October 21, 2010 at 8:26 pm
Jimmy,
Your depth of knowledge and understanding is beyond what most of us civilians can understand and comprehend, but you have valuable insights that you have been very willing to share with us. So I want to ask a few questions on behalf of those of us who are Stage IV, and either involved in or considering systemic immunotherapy. Your clearly are trying to help many of us by posting here, and have offered many people encouragement with your own story.
You have said that the most effective durable treatment for advanced melanoma would consist of Ipilimumab combined with IL2 – is that correct? There are no studies currently availble that combine Ipi and IL2, is that correct? If someone were to choose to do a combination treatment on their own (i.e. get IL2 following a course of Ipi through one of the clinical trials), would there be an advantage to starting IL2 as soon as possible after stopping Ipi? Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?
Last, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi?
Thank you so much for your assistance to this community.
Regards,
Jim
-
- October 21, 2010 at 8:26 pm
Jimmy,
Your depth of knowledge and understanding is beyond what most of us civilians can understand and comprehend, but you have valuable insights that you have been very willing to share with us. So I want to ask a few questions on behalf of those of us who are Stage IV, and either involved in or considering systemic immunotherapy. Your clearly are trying to help many of us by posting here, and have offered many people encouragement with your own story.
You have said that the most effective durable treatment for advanced melanoma would consist of Ipilimumab combined with IL2 – is that correct? There are no studies currently availble that combine Ipi and IL2, is that correct? If someone were to choose to do a combination treatment on their own (i.e. get IL2 following a course of Ipi through one of the clinical trials), would there be an advantage to starting IL2 as soon as possible after stopping Ipi? Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?
Last, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi?
Thank you so much for your assistance to this community.
Regards,
Jim
-
Tagged: cutaneous melanoma
- You must be logged in to reply to this topic.