› Forums › General Melanoma Community › $30K per dose!
- This topic has 58 replies, 21 voices, and was last updated 15 years, 4 months ago by
Rocco.
- Post
-
- March 25, 2011 at 7:14 pm
Excerpt from a Bloomberg.com article regarding the approval of ipi todayi….
Excerpt from a Bloomberg.com article regarding the approval of ipi todayi….
"The Food and Drug Administration cleared the medicine for patients with widely spread melanoma, the agency said today in a statement. The approval isn’t limited to patients who failed prior treatment, Bristol-Myers spokeswoman Tracy Furey said in a telephone interview today. Yervoy will cost $30,000 a dose, or $120,000 for a four-dose course of treatment, Furey said. "
$120K – I hope the insurance companies will foot this……
- Replies
-
-
- March 25, 2011 at 7:39 pm
Hi
Well, it was just time before BMS got their "payout" for IPI. It is kind of discouraging that $120K for 4 infusions. Chances the isurance companies will pick up this cost is probably slim. Particualrly, if pre-authorization is needed!
If insurance co. do not pay for cost, the average patient could not even pay for the drug at $120…..hell $30 K for1 infusion would be impossible for me to pay….somaybe getting this drug approved was not the best thing for patients. At least patients, had access through the compassionate use clincial trial.
What can we do???
-
- March 25, 2011 at 7:39 pm
Hi
Well, it was just time before BMS got their "payout" for IPI. It is kind of discouraging that $120K for 4 infusions. Chances the isurance companies will pick up this cost is probably slim. Particualrly, if pre-authorization is needed!
If insurance co. do not pay for cost, the average patient could not even pay for the drug at $120…..hell $30 K for1 infusion would be impossible for me to pay….somaybe getting this drug approved was not the best thing for patients. At least patients, had access through the compassionate use clincial trial.
What can we do???
-
- March 27, 2011 at 6:04 am
In 2006 High dose Interferon Therapy was the prescribed cure and it cost me $10,000 for 5 days and I was suppose to due 4 weeks….so that was $40,000 for a therapy that had been around for quite some time. Is it relevant? For the time yes.
The troubling aspect of this is for people who are on federal funded medicare and state funded medicade. You hear the Politicians talk about death panels. Well in 2006 I was emailing a lady in Tennessee who was on medicade, who was stage III and they State told her she was ineligible for interferon therapy…..medicade would not pay for it. What is that?
-
- March 27, 2011 at 6:04 am
In 2006 High dose Interferon Therapy was the prescribed cure and it cost me $10,000 for 5 days and I was suppose to due 4 weeks….so that was $40,000 for a therapy that had been around for quite some time. Is it relevant? For the time yes.
The troubling aspect of this is for people who are on federal funded medicare and state funded medicade. You hear the Politicians talk about death panels. Well in 2006 I was emailing a lady in Tennessee who was on medicade, who was stage III and they State told her she was ineligible for interferon therapy…..medicade would not pay for it. What is that?
-
- March 25, 2011 at 8:15 pm

My opinion is that Bristol Meyers is over-charging and taking advantage of the sick and dying. They are trying to compare themselves to "provenge" from Dendreon. Totally different.
When they scale up, they can make over 10,000 units a batch.
Supply and demand … What is your life worth?
Shame on BMY for taking advantage when we are down.
-
- March 25, 2011 at 8:15 pm
My opinion is that Bristol Meyers is over-charging and taking advantage of the sick and dying. They are trying to compare themselves to "provenge" from Dendreon. Totally different.
When they scale up, they can make over 10,000 units a batch.
Supply and demand … What is your life worth?
Shame on BMY for taking advantage when we are down.
-
- March 25, 2011 at 9:55 pm
WE (THE PATIENTS) TAKE ALL THE RISKS AND BRISTOL MYER SQUIBB REAPS THE REWARD.
VERY GREEDY AND UNETHICAL.
I am scientifically trying to find another way around controlling the Tregs so we can bypass Yervoy all together.
-
- March 25, 2011 at 9:55 pm
WE (THE PATIENTS) TAKE ALL THE RISKS AND BRISTOL MYER SQUIBB REAPS THE REWARD.
VERY GREEDY AND UNETHICAL.
I am scientifically trying to find another way around controlling the Tregs so we can bypass Yervoy all together.
-
- March 26, 2011 at 6:43 am
Jim, I admire your passion to the cure of disease. But, Charlies is right. Any company always want to be profitable. How many drugs are available for melanoma? and how many frequenly new drug come to available. Researchers and their staffs also have their family to support.. who pay for their bills? At one conference I attended, the doctors were worry about the limit of new antibiotic drugs available due to the natural change of the virus, bacteria. The doctors were worry that pharmaceutical companies would like to develop a drug like Viagra, or cholesterol so that they can sell for more profit.. but people can actually don't need it such they can excercise more often and eat healthy food. Look at the history, how many biotech companies have vanished when the drug fail. As you might know, the average cost to bring 1 drug to the market is 1 billion dollars. Long time ago, I was like you disagree with the cost of health care and drugs. But my view point had changed completely. That's true the charge is high, but how much any company has spent on the R&D, and how much they has lost with other products that fail to make the market? If they don't make profit, where they will get money to continue other R&D? I would rather to see them make profit and continue to develop a better drug, a better treatment… not only for melanoma, but also other cancers. Do you want all the pharmaceutical companies outsourcing their talents to China, like the high tech companies do, for cheaper price? Do you want every time you see a doctor.. by flying to China with their herb products? When you want a treatment, do you go to the best cancer center/hospital? If so, every thing must have a price.
-
- March 27, 2011 at 10:50 am
Yes, everything must have a price, but in all honesty too much money is wasted, before and after, to bring these drugs to fruition and as the FDA has shown in the past, by removing or reclassifying very effective natural chemicals to certain products, it is all about the the buck and politics, not people.
-
- March 27, 2011 at 10:50 am
Yes, everything must have a price, but in all honesty too much money is wasted, before and after, to bring these drugs to fruition and as the FDA has shown in the past, by removing or reclassifying very effective natural chemicals to certain products, it is all about the the buck and politics, not people.
-
- March 26, 2011 at 6:43 am
Jim, I admire your passion to the cure of disease. But, Charlies is right. Any company always want to be profitable. How many drugs are available for melanoma? and how many frequenly new drug come to available. Researchers and their staffs also have their family to support.. who pay for their bills? At one conference I attended, the doctors were worry about the limit of new antibiotic drugs available due to the natural change of the virus, bacteria. The doctors were worry that pharmaceutical companies would like to develop a drug like Viagra, or cholesterol so that they can sell for more profit.. but people can actually don't need it such they can excercise more often and eat healthy food. Look at the history, how many biotech companies have vanished when the drug fail. As you might know, the average cost to bring 1 drug to the market is 1 billion dollars. Long time ago, I was like you disagree with the cost of health care and drugs. But my view point had changed completely. That's true the charge is high, but how much any company has spent on the R&D, and how much they has lost with other products that fail to make the market? If they don't make profit, where they will get money to continue other R&D? I would rather to see them make profit and continue to develop a better drug, a better treatment… not only for melanoma, but also other cancers. Do you want all the pharmaceutical companies outsourcing their talents to China, like the high tech companies do, for cheaper price? Do you want every time you see a doctor.. by flying to China with their herb products? When you want a treatment, do you go to the best cancer center/hospital? If so, every thing must have a price.
-
- March 26, 2011 at 3:40 am
I'm a bit surprised about your position, Jim. If I understand your resume', you were a researcher for Eastman Kodak.
Did you work for free? Did you go to work everyday simply for the good of mankind and toil away, all the while going home content that even though you did good, you have no need to be compensated for your efforts and contribution?
Who paid for the building for the lab you worked in? Who paid for the lab equipment and the lab assistants? Who paid the water, sewer, electric, gas, trash and insurance bill? Who paid the payroll clerk to track your time worked, buy the paper checks, write the checks, balance the checkbook so your paycheck didn;t bounce, who paid the accountant to make certain your payroll taxes were computed correctly, who paid to make sure your payroll deductions were forwarded to the state and federal level?
Did your company pay for product development, prove scientific research that was able to be duplicated, engineering, patents, copyrights, marketing, advertising, manufacturing design, , distribution, legal, accounting and product liability and federal approval for distribution and then give the end product away ?
I don't think so.
I guess we should all get out our erector sets and chemistry sets, go out in the garage and mix something up and do it ourselves, huh? That way, it wouldn't cost anything……………………and we could alllllllllllllllllllllllll give it away.
Take a simple doctors appointment. First the doctor has to pay to get an education, get credentialed, buy or rent a building, and get a license and insurance and equipment. Then, when you call, their is the cost of a phone line, paying someone to answer your call, the cost of the desk, chair, and when you are transferred to the appointment clerk, that person has to be paid, that person will enter your information into a computer that must be paid for and recorded into your records, which must be stored in a paper file that requires a printer, paper, ink, a file folder and somebody has to be paid to guard that file.
Then, when you actually get to your appointment, the check in desk person (paid), passes your insurance information to the insurance person (paid) who verifies you coverage with the insurance people (some one is paid there), then you see a nurse (paid) who enters information in your file, which someone was paid to retreive, weighs you(after buying the scales), checks your blood pressure(with the cuff that had to be purchased), maybe a blood draw (the phlebotomist is paid) to stick a needle in you(which someone had to buy), put a label on it(which somebody had to buy) and send it to a lab(which someone has paid for) to a lab tech, who has to be paid, and……………well I hope you get the idea.
It is unrealistic to expect a pharma company not to want to recoup their costs. No, I am NOT a big fan of big pharma, but if they don't develop the treatment drugs, who will?
More so, who is going to do that for free?
Nobody, that's who.
Quit your bitchin.
Charlie S
-
- March 26, 2011 at 4:06 am
We are hopeful that Insurance will cover the expense of IPI, that being said, Charlie do you suffer from Stage IV Metastatic Melanoma? I don't like your tone at all. When you are dying and have no energy, but want desparately to live…..and here is IPI FDA approved…how would you feel if you couldn't afford to pay. Until you are near your last breath like so many of us are, don't be so callous. No one would complain if they had the money to pay for this. We all want a chance to live.
-
- March 26, 2011 at 4:28 am
Actually, you should probably just click on Charlie's name and see that he is a chronic stage IV melanoma warrior. He's been through plenty and has had his own near misses. His "love", a member of this community, also passed away from melanoma. So his opinion is very valid as a stage IV patient and caregiver.
The reality is that drugs are incredibly expensive to develop. Years of research, years of trials, expensives just to comply with the FDA regulations. Heck, even compassionate use costs $$$. I don't know if anyone can really appreciate the scope of what goes into this. I've seen personally what goes into an FDA submission for a medical device and it's unbelievable. We may not like it, but it's understandable the cost of the drugs. And what about the other drugs they research and try to make work for melanoma — that may fail the trials? Those just don't come free either. There are few cancer treatments that we can afford without insurance. I may not like it, I may not agree with it, but I understand it. If I want free cancer treatments, I will have to move to a country with socialized medicine. Free or even affordable isn't going to happen in the US with the scope of these types of medicines.
Just my 2 cents.
-
- March 26, 2011 at 4:28 am
Actually, you should probably just click on Charlie's name and see that he is a chronic stage IV melanoma warrior. He's been through plenty and has had his own near misses. His "love", a member of this community, also passed away from melanoma. So his opinion is very valid as a stage IV patient and caregiver.
The reality is that drugs are incredibly expensive to develop. Years of research, years of trials, expensives just to comply with the FDA regulations. Heck, even compassionate use costs $$$. I don't know if anyone can really appreciate the scope of what goes into this. I've seen personally what goes into an FDA submission for a medical device and it's unbelievable. We may not like it, but it's understandable the cost of the drugs. And what about the other drugs they research and try to make work for melanoma — that may fail the trials? Those just don't come free either. There are few cancer treatments that we can afford without insurance. I may not like it, I may not agree with it, but I understand it. If I want free cancer treatments, I will have to move to a country with socialized medicine. Free or even affordable isn't going to happen in the US with the scope of these types of medicines.
Just my 2 cents.
-
- March 27, 2011 at 10:55 am
A chance to live?? four months for 120k?? with a chance of fatal side effects, after paying for the treatment?? Four more months of living with the immunosuppressant fear of the inevitable?? I don't know…..
-
- March 27, 2011 at 10:55 am
A chance to live?? four months for 120k?? with a chance of fatal side effects, after paying for the treatment?? Four more months of living with the immunosuppressant fear of the inevitable?? I don't know…..
-
- March 26, 2011 at 4:06 am
We are hopeful that Insurance will cover the expense of IPI, that being said, Charlie do you suffer from Stage IV Metastatic Melanoma? I don't like your tone at all. When you are dying and have no energy, but want desparately to live…..and here is IPI FDA approved…how would you feel if you couldn't afford to pay. Until you are near your last breath like so many of us are, don't be so callous. No one would complain if they had the money to pay for this. We all want a chance to live.
-
- March 26, 2011 at 4:39 am
You must be new here, A. I can answer your question in your first sentence: a resounding YES, Charlie has Stage IV melanoma. You must be new here to not know of Charlie. I am astounded, too, over the dollar signs attached to this drug, but I followed the train of thought that Charlie pointed out in such detail. I don't know where this will go, how it will go—-I'm just glad it IS going in a forward direction, finally.
CarolA
Stage III & holding
-
- March 26, 2011 at 4:39 am
You must be new here, A. I can answer your question in your first sentence: a resounding YES, Charlie has Stage IV melanoma. You must be new here to not know of Charlie. I am astounded, too, over the dollar signs attached to this drug, but I followed the train of thought that Charlie pointed out in such detail. I don't know where this will go, how it will go—-I'm just glad it IS going in a forward direction, finally.
CarolA
Stage III & holding
-
- March 26, 2011 at 3:27 pm
Charlie,
Is there such a thing as their fair share. The price is excessive.
There is a Drug on the market that does the same thing for 750.00 /24 doses. You may have heard of it Imiquimod , Aldera from Graceway Pharmaceuticals . It is a prescription medication that acts as an immune response modifier.
That is what Ipilimumab does, it modifies the immune system.
It has been use as off-label use for Melanoma and has been very successful. Only 750.00. BMY is sell you snake oil at 3mg/kg. The optimal dose concentration is 10 mg/kg based on a trial by Dr. Jedd Wolchok. IT is the water down version
I myself had a dose of 15mg/kg of Pfizer's Anti-CTLA-4 drug.
All I am trying to say is the price is too excessive. I believe 20000 a dose is more realistic and fair. That is my opinion.
10mg/kg with 4 doses at 120000 is fair!!!!!!
Best regards,
jimmy B
-
- March 26, 2011 at 11:05 pm
Hi Jim,
Of note is that my oncologist said that when they participated in the Ipi trial a few years ago with the dose being higher (?10mg/kg) than what I got (3mg/kg) they had more patient deaths from the severe side effects, most often the colitis. They were seeing favorable results in many patients at the 3kg/mg with much fewer side effects. Time will tell whether I will have a durable response. I hope I do.
Vermont_Donna
-
- March 26, 2011 at 11:05 pm
Hi Jim,
Of note is that my oncologist said that when they participated in the Ipi trial a few years ago with the dose being higher (?10mg/kg) than what I got (3mg/kg) they had more patient deaths from the severe side effects, most often the colitis. They were seeing favorable results in many patients at the 3kg/mg with much fewer side effects. Time will tell whether I will have a durable response. I hope I do.
Vermont_Donna
-
- March 26, 2011 at 3:27 pm
Charlie,
Is there such a thing as their fair share. The price is excessive.
There is a Drug on the market that does the same thing for 750.00 /24 doses. You may have heard of it Imiquimod , Aldera from Graceway Pharmaceuticals . It is a prescription medication that acts as an immune response modifier.
That is what Ipilimumab does, it modifies the immune system.
It has been use as off-label use for Melanoma and has been very successful. Only 750.00. BMY is sell you snake oil at 3mg/kg. The optimal dose concentration is 10 mg/kg based on a trial by Dr. Jedd Wolchok. IT is the water down version
I myself had a dose of 15mg/kg of Pfizer's Anti-CTLA-4 drug.
All I am trying to say is the price is too excessive. I believe 20000 a dose is more realistic and fair. That is my opinion.
10mg/kg with 4 doses at 120000 is fair!!!!!!
Best regards,
jimmy B
-
- March 26, 2011 at 3:40 am
I'm a bit surprised about your position, Jim. If I understand your resume', you were a researcher for Eastman Kodak.
Did you work for free? Did you go to work everyday simply for the good of mankind and toil away, all the while going home content that even though you did good, you have no need to be compensated for your efforts and contribution?
Who paid for the building for the lab you worked in? Who paid for the lab equipment and the lab assistants? Who paid the water, sewer, electric, gas, trash and insurance bill? Who paid the payroll clerk to track your time worked, buy the paper checks, write the checks, balance the checkbook so your paycheck didn;t bounce, who paid the accountant to make certain your payroll taxes were computed correctly, who paid to make sure your payroll deductions were forwarded to the state and federal level?
Did your company pay for product development, prove scientific research that was able to be duplicated, engineering, patents, copyrights, marketing, advertising, manufacturing design, , distribution, legal, accounting and product liability and federal approval for distribution and then give the end product away ?
I don't think so.
I guess we should all get out our erector sets and chemistry sets, go out in the garage and mix something up and do it ourselves, huh? That way, it wouldn't cost anything……………………and we could alllllllllllllllllllllllll give it away.
Take a simple doctors appointment. First the doctor has to pay to get an education, get credentialed, buy or rent a building, and get a license and insurance and equipment. Then, when you call, their is the cost of a phone line, paying someone to answer your call, the cost of the desk, chair, and when you are transferred to the appointment clerk, that person has to be paid, that person will enter your information into a computer that must be paid for and recorded into your records, which must be stored in a paper file that requires a printer, paper, ink, a file folder and somebody has to be paid to guard that file.
Then, when you actually get to your appointment, the check in desk person (paid), passes your insurance information to the insurance person (paid) who verifies you coverage with the insurance people (some one is paid there), then you see a nurse (paid) who enters information in your file, which someone was paid to retreive, weighs you(after buying the scales), checks your blood pressure(with the cuff that had to be purchased), maybe a blood draw (the phlebotomist is paid) to stick a needle in you(which someone had to buy), put a label on it(which somebody had to buy) and send it to a lab(which someone has paid for) to a lab tech, who has to be paid, and……………well I hope you get the idea.
It is unrealistic to expect a pharma company not to want to recoup their costs. No, I am NOT a big fan of big pharma, but if they don't develop the treatment drugs, who will?
More so, who is going to do that for free?
Nobody, that's who.
Quit your bitchin.
Charlie S
-
- March 25, 2011 at 11:01 pm
The attitude of all of you really makes me feel crappy.
I'm lucky to be a responder so I'm a bit slanted. Sit down and figure out the cost of the reasearch that went into a drug like this. Not just this drug but the braf's and mek inhibitors, IL-2.
Who paid for compassionate use drugs? How long do you want any company to wait for a repayment of investment.
Let's just nationalize insurance and we will have all the benefits and availablity that our neighbors to the north and those across the big pond.
You sound like a bunch of gimmee, gimmee, gimmee's, but you also DEMAND that you get product.
I'm outta here.
You can have at me, cause I'm not coming back to such a negative place.
Jerry from Cape Cod – Gone
-
- March 25, 2011 at 11:01 pm
The attitude of all of you really makes me feel crappy.
I'm lucky to be a responder so I'm a bit slanted. Sit down and figure out the cost of the reasearch that went into a drug like this. Not just this drug but the braf's and mek inhibitors, IL-2.
Who paid for compassionate use drugs? How long do you want any company to wait for a repayment of investment.
Let's just nationalize insurance and we will have all the benefits and availablity that our neighbors to the north and those across the big pond.
You sound like a bunch of gimmee, gimmee, gimmee's, but you also DEMAND that you get product.
I'm outta here.
You can have at me, cause I'm not coming back to such a negative place.
Jerry from Cape Cod – Gone
-
- March 26, 2011 at 12:15 am
Don't leave Jerry.
Jerry has a good point….they have to recoup all of the R & D money and then some.
Many may be overreacting too.
Don't assume that insurance will not pay for it and if they don't, that the cost will be $30,000 per dose out of your pocket.
A lot needs to come out yet.
I hope that you stay around, Jerry.
-
- March 26, 2011 at 12:15 am
Don't leave Jerry.
Jerry has a good point….they have to recoup all of the R & D money and then some.
Many may be overreacting too.
Don't assume that insurance will not pay for it and if they don't, that the cost will be $30,000 per dose out of your pocket.
A lot needs to come out yet.
I hope that you stay around, Jerry.
-
- March 26, 2011 at 1:56 am
While this allows for more access to more people….it won't be free in trials anymore…and the cost is crazy…most stage 4 patients who need this are not working….
I had Temodar and after blue cross and blue shield they still wanted me to pay over 1800 a month….when I took it 5 days every 28 and I thought that was bad…
-
- March 26, 2011 at 3:29 pm
Hi All,
For what it is worth, I contacted my Blue Shield of CA (spoke to Manager over Benefits) regarding coverage to pay for IPI. I was told that the fact FDA approved IPI there was no guarantee the Blue Shield would pay for the drug. Patients would have to get a pre-service authoriztion which entails reviewing patients history then Blue Shield would make a decision whether or not to pay for the drug.
Well, the review of patient's history is a reasonable process to determine coverage on IPI. But then I was told that IPI is so new, that the decision to pay for IPI was very low because the drug was so NEW & the drug is considered experimental/investigatory at this stage…not enough patients took the drug on the clinical trials
For those now on the drug under compassionate use,your chances are better to get payment for IPI because you are in the middle of treatment. For those, hoping to start IPI, it will be an up hill battle with Blue Shield.
I asked if IPI covered under Medicare would that make a difference that Blue Shield would pay for IPI. The manager told me "NO". For those not covered under Medicare, our chances of getting IPI paid for by insurance could be problematic.
I read another post on MPIP that said, maybe we were better off having IPI under compassionate use because now it is up to insurance companier whether or not to pay for IPI. I think that is a worse situation than trying to get IPI under compassionate use. Now our fate is up to the insurance companies. Life is not easy.
Thanks for taking the time to read my post
Douglas
-
- March 26, 2011 at 3:36 pm
-
- March 26, 2011 at 3:36 pm
-
- March 26, 2011 at 3:29 pm
Hi All,
For what it is worth, I contacted my Blue Shield of CA (spoke to Manager over Benefits) regarding coverage to pay for IPI. I was told that the fact FDA approved IPI there was no guarantee the Blue Shield would pay for the drug. Patients would have to get a pre-service authoriztion which entails reviewing patients history then Blue Shield would make a decision whether or not to pay for the drug.
Well, the review of patient's history is a reasonable process to determine coverage on IPI. But then I was told that IPI is so new, that the decision to pay for IPI was very low because the drug was so NEW & the drug is considered experimental/investigatory at this stage…not enough patients took the drug on the clinical trials
For those now on the drug under compassionate use,your chances are better to get payment for IPI because you are in the middle of treatment. For those, hoping to start IPI, it will be an up hill battle with Blue Shield.
I asked if IPI covered under Medicare would that make a difference that Blue Shield would pay for IPI. The manager told me "NO". For those not covered under Medicare, our chances of getting IPI paid for by insurance could be problematic.
I read another post on MPIP that said, maybe we were better off having IPI under compassionate use because now it is up to insurance companier whether or not to pay for IPI. I think that is a worse situation than trying to get IPI under compassionate use. Now our fate is up to the insurance companies. Life is not easy.
Thanks for taking the time to read my post
Douglas
-
- March 26, 2011 at 1:56 am
While this allows for more access to more people….it won't be free in trials anymore…and the cost is crazy…most stage 4 patients who need this are not working….
I had Temodar and after blue cross and blue shield they still wanted me to pay over 1800 a month….when I took it 5 days every 28 and I thought that was bad…
-
- March 26, 2011 at 10:25 pm
No real surprises here, so let's please be civil in discussions about this drug and others coming along. I have my own issues with the system, but will save those for another day. What just happened is that BMY announced pricing to begin negotiations with insurers and other large customers (governments here and abroad) about what they will pay. The decision makers who determine "formularies" will feel compelled to include it as a new "standard of care" along with one or more of the BRAF treatments. The buyers should be able to negotiate the price down significantly to $15,000 or so, or maybe $10,000. If you are more than a casual observerer about how Pharma operates, than what is happening should be no surprise. BMY attempting to "sit on" MDX1106 and 1105 should perhaps be an even larger concern for the Melanoma community, since they each look more promising than Ipi/Yervoy/MDX010. The system and players in it may be flawed, but it is the only system we have in the US for now – for better or worse (or both). BMY will try to minimize PR blowback with discounting and assistance for those who lack insurance and sufficient resources, or the combination.
The fact that BMY attempting to "sit on" MDX1106 and 1105 should perhaps be an even larger concern for the Melanoma community, since they each look more promising than Ipi/Yervoy/MDX010. BMY first wants to recover its costs of developing Ipi, which is rational from their business standpoint, but not defensible from a medical and ethical standpoint. I have my own issues with the system, but will save those for another day.
Best to All,
Jim
-
- March 26, 2011 at 11:02 pm
Jim,
It is good to hear from you. You are right Anti-PD-1 looks very promising.
Dr. Rafi Ahmed is now being introduced by Johannes Vieweg, & highlighting his work on immunological memory
Dr. Ahmed is sharing how lessons from immune memory development in chronic viral infection can inform cancer immunotherapy field
Ahmed: wait 30-60 days to boost in vaccination produces better immune responses for many types of viral vaccines. Same for cancer?
Ahmed: too frequent boosting causes T cells to differentiate too far into their cell-death cycle — so you lose potency of vaccines
Ahmed: immune exhaustion in chronic infection requires boost to CD4 T cells – critical to protection in chronic-not acute-infection
Strategies in cancer immunotherapy should consider how to rescue fatigued T cells that have been over-exposed to cancer antigen
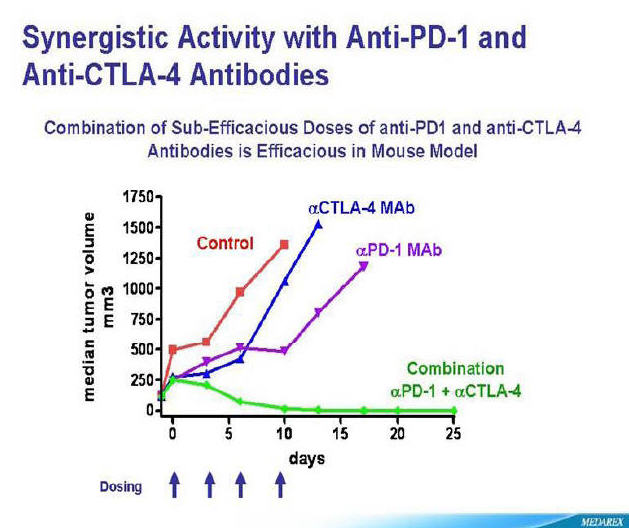
Ahmed: anti-PD-1 therapy may help to rescue fatigued CD8 T cells in chronic viral infection and cancer immunotherapy
Ahmed: PD-1 is a significant player in regulating T-cell exhaustion in chronic infection and cancer. Combo therapy needed.
Ahmed: Synergy we've seen combining PD-1 with IL-2 (negative + positive signal) in viral infection therapy have been astonishing.
-
- March 26, 2011 at 11:02 pm
Jim,
It is good to hear from you. You are right Anti-PD-1 looks very promising.
Dr. Rafi Ahmed is now being introduced by Johannes Vieweg, & highlighting his work on immunological memory
Dr. Ahmed is sharing how lessons from immune memory development in chronic viral infection can inform cancer immunotherapy field
Ahmed: wait 30-60 days to boost in vaccination produces better immune responses for many types of viral vaccines. Same for cancer?
Ahmed: too frequent boosting causes T cells to differentiate too far into their cell-death cycle — so you lose potency of vaccines
Ahmed: immune exhaustion in chronic infection requires boost to CD4 T cells – critical to protection in chronic-not acute-infection
Strategies in cancer immunotherapy should consider how to rescue fatigued T cells that have been over-exposed to cancer antigen
Ahmed: anti-PD-1 therapy may help to rescue fatigued CD8 T cells in chronic viral infection and cancer immunotherapy
Ahmed: PD-1 is a significant player in regulating T-cell exhaustion in chronic infection and cancer. Combo therapy needed.
Ahmed: Synergy we've seen combining PD-1 with IL-2 (negative + positive signal) in viral infection therapy have been astonishing.
-
- March 26, 2011 at 10:25 pm
No real surprises here, so let's please be civil in discussions about this drug and others coming along. I have my own issues with the system, but will save those for another day. What just happened is that BMY announced pricing to begin negotiations with insurers and other large customers (governments here and abroad) about what they will pay. The decision makers who determine "formularies" will feel compelled to include it as a new "standard of care" along with one or more of the BRAF treatments. The buyers should be able to negotiate the price down significantly to $15,000 or so, or maybe $10,000. If you are more than a casual observerer about how Pharma operates, than what is happening should be no surprise. BMY attempting to "sit on" MDX1106 and 1105 should perhaps be an even larger concern for the Melanoma community, since they each look more promising than Ipi/Yervoy/MDX010. The system and players in it may be flawed, but it is the only system we have in the US for now – for better or worse (or both). BMY will try to minimize PR blowback with discounting and assistance for those who lack insurance and sufficient resources, or the combination.
The fact that BMY attempting to "sit on" MDX1106 and 1105 should perhaps be an even larger concern for the Melanoma community, since they each look more promising than Ipi/Yervoy/MDX010. BMY first wants to recover its costs of developing Ipi, which is rational from their business standpoint, but not defensible from a medical and ethical standpoint. I have my own issues with the system, but will save those for another day.
Best to All,
Jim
-
- March 26, 2011 at 10:59 pm
I am really sad to see that this thread has turned in to personally attacking people for stating their opinion. It's okay to disagree but why attack someone personally. And if I don't agree with your opinion why is that considered to be "negativity". I thought that open discussions where for everyone to state their point of view.
I've never seen this happen on this board like I have others. Aren't we all entitled to our opinion?
JillNEric in OH
-
- March 26, 2011 at 10:59 pm
I am really sad to see that this thread has turned in to personally attacking people for stating their opinion. It's okay to disagree but why attack someone personally. And if I don't agree with your opinion why is that considered to be "negativity". I thought that open discussions where for everyone to state their point of view.
I've never seen this happen on this board like I have others. Aren't we all entitled to our opinion?
JillNEric in OH
-
- March 27, 2011 at 12:34 am
My husband, Earl, died 3 weeks ago. Stage 4 melanoma which led to liver failure. He was too sick to qualify for the ipi trial, but died before the approval. How I wish he couId be here, starting this medication, while I would struggle to figure out how to pay the cost.
Rachel
-
- March 27, 2011 at 12:34 am
My husband, Earl, died 3 weeks ago. Stage 4 melanoma which led to liver failure. He was too sick to qualify for the ipi trial, but died before the approval. How I wish he couId be here, starting this medication, while I would struggle to figure out how to pay the cost.
Rachel
-
- March 27, 2011 at 4:54 am
Lots of posts, lots of disagreement. We don't even know if our insurance companies will pay or not, only time will tell. I do agree with the post that said that our companies will not be paying full amounts, this will be negotiated.
The number of people that could get compassionate care was limited. Not everyone can travel, we don't all live near large cancer centers. I immediately think of Charles from Nebraska. He has stated several times that he cannot travel and there is nothing that can be offered to him because of his heart issues. Many on this board have suggested that he travels to a center that offers ippi, even after he has stated that he cannot travel. Now him and many like him that live in rural areas will have a chance to have this drug.
We complain that the drug companies overlook melanoma when doing their research because we have a cancer that effects less people. They are a business and they will only be around to do more research if it is paid for! When something new comes out for breast cancer then many will be buying it, that equals profit. Since the amount of people buying ippi isn't as large then we have to pay the price. That's simple economics. They've said they will help those that can't afford the meds because of lack of insurance and help with co-pays for those who do have insurance but don't have the resources to pay. Someone has to pay for this!
Can I afford $120,000? No, I would need help, if my insurance company would pay for 80% then I could figure a way. Am I stage IV? Yes. My Dr. and I have discussed Ippi and since I haven't failed a treatment I was told that I would be put on something else for a month or so to prove that I failed it to get into the compassionate trial. As it turned out my latest nodule stabilized for now so I didn't have to try something just to get ippi like many on this board had to do.
Think of how many people got compassionate care ippi with no charge. A year ago everyone was screaming mad at the pharm people when they pulled it for awhile. Now your screaming because they are not continuing to provide without compensation.
My last scans were almost $15,000! Many have to figure out a way to pay for their scans without insurance, however when we talk about nationalized insurance most go crazy. How about if for at least a few days we are thankful that we now have a drug that has been recognized to help some of us. Maybe new ones will be coming to help more but research does cost.
I wish it cost less, but seriously, if it ended up costing $80.000 would that really make a difference to most of us? It would still be out of the common person's range.
Linda
-
- March 27, 2011 at 4:54 am
Lots of posts, lots of disagreement. We don't even know if our insurance companies will pay or not, only time will tell. I do agree with the post that said that our companies will not be paying full amounts, this will be negotiated.
The number of people that could get compassionate care was limited. Not everyone can travel, we don't all live near large cancer centers. I immediately think of Charles from Nebraska. He has stated several times that he cannot travel and there is nothing that can be offered to him because of his heart issues. Many on this board have suggested that he travels to a center that offers ippi, even after he has stated that he cannot travel. Now him and many like him that live in rural areas will have a chance to have this drug.
We complain that the drug companies overlook melanoma when doing their research because we have a cancer that effects less people. They are a business and they will only be around to do more research if it is paid for! When something new comes out for breast cancer then many will be buying it, that equals profit. Since the amount of people buying ippi isn't as large then we have to pay the price. That's simple economics. They've said they will help those that can't afford the meds because of lack of insurance and help with co-pays for those who do have insurance but don't have the resources to pay. Someone has to pay for this!
Can I afford $120,000? No, I would need help, if my insurance company would pay for 80% then I could figure a way. Am I stage IV? Yes. My Dr. and I have discussed Ippi and since I haven't failed a treatment I was told that I would be put on something else for a month or so to prove that I failed it to get into the compassionate trial. As it turned out my latest nodule stabilized for now so I didn't have to try something just to get ippi like many on this board had to do.
Think of how many people got compassionate care ippi with no charge. A year ago everyone was screaming mad at the pharm people when they pulled it for awhile. Now your screaming because they are not continuing to provide without compensation.
My last scans were almost $15,000! Many have to figure out a way to pay for their scans without insurance, however when we talk about nationalized insurance most go crazy. How about if for at least a few days we are thankful that we now have a drug that has been recognized to help some of us. Maybe new ones will be coming to help more but research does cost.
I wish it cost less, but seriously, if it ended up costing $80.000 would that really make a difference to most of us? It would still be out of the common person's range.
Linda
-
- March 27, 2011 at 10:55 am
I was handed a copy of an internal BMS email that was widely distributed to US employees on Friday, March 25th right after the FDA approval. The email from the BMS CEO, Lamberto Andreotti included a high level overview of the FDA approval, the stats of the number of cases of mel per year, thanked the employees of both BMS and those from Medarex that made this day possible, etc. The email also included these 2 paragraph below. The underline and bold were my adds:
"Now patients in the U.S. with this devasting unmet medical need will have somewhere to trun. Distribution and sales of Yervoy will begin in the next few weeks. Virually all uninsured patients will be able to obtain the medicine free-of-charge through our robust oncology patient assistance program".
"Outside of the U.S. I look forward to Yervoy's future approval in other countries in the near future. Meanwhile, we will continue the expanded access / compassionate use program that has alreadhy benefitted more than 4,500 patients throughout the world."
-
- March 27, 2011 at 10:55 am
I was handed a copy of an internal BMS email that was widely distributed to US employees on Friday, March 25th right after the FDA approval. The email from the BMS CEO, Lamberto Andreotti included a high level overview of the FDA approval, the stats of the number of cases of mel per year, thanked the employees of both BMS and those from Medarex that made this day possible, etc. The email also included these 2 paragraph below. The underline and bold were my adds:
"Now patients in the U.S. with this devasting unmet medical need will have somewhere to trun. Distribution and sales of Yervoy will begin in the next few weeks. Virually all uninsured patients will be able to obtain the medicine free-of-charge through our robust oncology patient assistance program".
"Outside of the U.S. I look forward to Yervoy's future approval in other countries in the near future. Meanwhile, we will continue the expanded access / compassionate use program that has alreadhy benefitted more than 4,500 patients throughout the world."
-
- You must be logged in to reply to this topic.